
NCPSSM Makes Final Endorsements of 2022 Cycle, Emphasizing GOP Threats to Social Security and Medicare

As the midterm campaign draws to a close with the future of Social Security and Medicare possibly at stake, NCPSSM has been completing its final round of candidate endorsement events around the country. Today in Charlotte, North Carolina, NCPSSM legislative director and PAC coordinator Dan Adcock formally endorsed Democrat Cheri Beasley for U.S. Senate in one of the pivotal swing state races of this election cycle.
Adcock presented Beasley with the National Committee’s signature boxing gloves, symbolizing that she is a “champion” for seniors in North Carolina. Beasley, the former Chief Justice of North Carolina’s Supreme Court, is running against Republican congressman Ted Budd for the seat currently held by GOP Sen. Richard Burr. The outcome of this race could determine who controls the Senate come January.
“Cheri Beasley will protect and improve Social Security. Her opponent voted for a budget proposal that would have cut COLAs and raised the retirement age to 70. Cheri Beasley will protect and improve Medicare. Ted Budd voted to privatize Medicare for the benefit of insurance companies.” – NCPSSM legislative director and PAC coordinator Dan Adcock, Charlotte, NC, 11/4/22
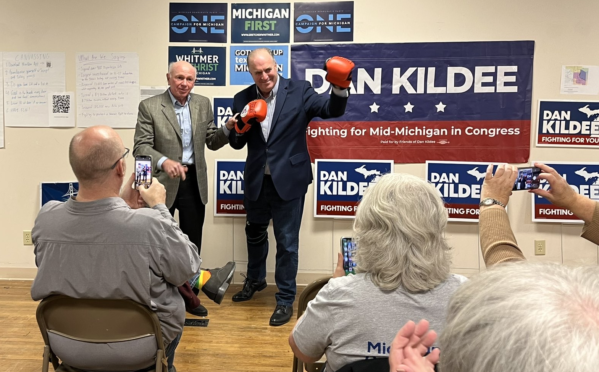
The National Committee has endorsed nearly 100 candidates across the U.S. for House and Senate this year. On Thursday, NCPSSM president Max Richtman was in Bay City, MI, endorsing Rep. Dan Kildee (D-IL) for re-election to the U.S. House, pronouncing him the “Rocky Balboa” for older Michiganders.
“Every step of the way, Dan Kildee has made the right call. He voted dozens of times to protect the Affordable Care Act while Republicans were hellbent on overturning it, stripping Michiganders with pre-existing conditions of their health care coverage and kicking millions off of Medicaid. And since Representative Kildee first took office, he has been a leader in the fight to improve Social Security and Medicare and reduce health care costs.” – Max Richtman, 11/3/22
Richtman also commended Rep. Kildee for his leadership on the House Ways and Means Social Security subcommittee, saying it’s important that he remain in that role to help protect senior’s earned benefits.
On Saturday, Richtman will be in Ohio to throw the National Committee’s support behind U.S. Rep Tim Ryan (D-OH) in his bid to defeat Republican J.D. Vance for the seat being vacated by Sen. Rob Portman (R-OH). While key Republicans have proposed harmful proposals for seniors’ earned benefits, Vance appears to have moderated his stance about Social Security and Medicare since running for this seat:
“His Democratic opponent, Rep. Tim Ryan, has criticized Vance for a 2010 blog post that described Social Security and Medicare among the largest drivers of the deficit. But Vance has since downplayed the need for changes to the programs.” – Bloomberg Government, 10/31/22
Meanwhile, Rep. Ryan has been a staunch ally of seniors in the U.S. Congress and earned a 100% rating on NCPSSM’s legislative scorecard. He has fought back against efforts to cut and privatize Social Security and Medicare – and “has supported legislation that would put more money in seniors’ pockets by increasing benefits, cutting taxes, and ensuring that Social Security keeps up with the rising cost of living.” Ryan also supports strengthening and expanding Medicare.
The mid-term election has become an existential threat for the nation’s two main social insurance programs for seniors, with Republicans openly proposing to cut, privatize, or jeopardize Social Security and Medicare. President Biden couldn’t have put it more plainly during a speech in Florida this week:
“You’ve been paying into (these programs) your whole life. You earned it. Now these guys want to take it away. Who in the hell do they think they are?” – President Biden, 11/1/22
NCPSSM has been calling on senior voters to cast ballots in their own interest, emphasizing that the GOP is not worthy of their trust on these issues – and that Republicans have no productive plans for addressing high priority items like inflation and gas prices. As Los Angeles Times Michael Hiltzik columnist recently wrote in a piece entitled, Republicans Keep Harping on Inflation, But Don’t Have Any Answers for It: “Proposals to diminish seniors’ benefits in any way would make it even harder for older Americans to cope with today’s economic difficulties.”
On Tuesday, voters will have an opportunity to protect their financial and health security – or take a risky step toward losing the programs that have ensured those very things for generations.
Let’s Protect Social Security & Medicare On November 8th

It is no exaggeration to say that the nation’s two most important programs for seniors—Social Security and Medicare—are on the line in this November’s elections. This is not a matter of nuance; it’s truly existential. Whichever party controls Congress will influence whether Social Security and Medicare will continue as we know them—or be weakened and privatized. The outcome depends largely on how older Americans—who cast ballots more reliably than any other age group—vote in 2022.
For seniors, the stakes could not be higher, nor the choice clearer. “The Social Security you paid for from the time you had a job is on the ballot. Your right to vote is on the ballot. Even the democracy. Are you ready to fight for these things now?” said President Joe Biden at an August rally in Maryland.
The president was not exaggerating. Democrats have made earnest efforts to boost Social Security and Medicare in the 117th Congress—and to shore up the finances of both programs. They have introduced legislation in both the House and Senate to strengthen Social Security and expand benefits. Democrats passed the Inflation Reduction Act, which should significantly lower seniors’ prescription drug costs, with zero Republican support. Meanwhile, GOP members of Congress, who for years have mouthed general support for Social Security and Medicare, are now saying the quiet part out loud: They propose to break the fundamental promises of both programs.
You have to give Republicans credit for political brazenness, though perhaps recklessness is a better word. During an election year, Senator Rick Scott (R-Fla.), chair of the committee responsible for electing Republicans to the Senate, proposed a plan where Social Security and Medicare would have to be renewed every five years by Congress—putting both programs on a path toward steep budget cuts, if not outright elimination. Scott’s proposal garnered significant backlash, but that did not stop Senator Ron Johnson (R-Wisc.) from saying a few months later that Social Security and Medicare should be considered “discretionary” spending, placing seniors’ benefits at the mercy of the Congressional budget process every year.
Some Republican candidates for Congress have followed this path off the political cliff. As NBC News reported, “In major Senate and House races across the country, GOP candidates have called for cutting long-term Social Security spending to tackle inflation and resolve the program’s finances.” In Arizona, a state with one of the largest populations of retirees in the country, GOP Senate candidate Blake Masters endorsed the idea of gambling seniors’ earned benefits on the stock market. “Maybe we should privatize Social Security, right? Private retirement accounts, get the government out of it,” he said. Privatization is a terrible idea and a largely unpopular one, but conservative idealogues continue to push policies that are great for Wall Street, but harmful to seniors on fixed incomes.
Last June, the House Republican Study Committee’s budget blueprint included raising Social Security’s full retirement age—a massive benefit cut that ignores the fact that although some people are living longer, many are not able to continue working until age 70. The full retirement age has already been raised to 67 for anyone born in 1960 or later. Workers claiming Social Security before their full retirement age face reduced monthly benefits for life. Nearly half of retirees rely on Social Security for all or most of their income. The last thing they need is another increase in the retirement age—though this is one of the most popular ideas in Republican circles.
Social Security and Medicare are Democratic legacies, enacted by Democratic majorities in Congress and signed into law by Presidents Franklin D. Roosevelt and Lyndon B. Johnson, respectively. Democrats realize that both programs face financing challenges. Social Security’s combined trust fund is projected to become depleted by 2035 if Congress fails to take preventative action. The Medicare Part A trust fund will run out in 2028 without congressional help. While Republicans want future seniors to bear the burden of shoring up Social Security’s finances, Representative John Larson (D-Conn.) and Senator Bernie Sanders (I-Vt.), among others, champion solutions that produce more revenue, such as asking the wealthy to contribute their fair share in payroll taxes—allowing an actual boost in benefits.
Social Security and Medicare are not the only issues affecting seniors, who bore much of the brunt of the COVID-19 pandemic both in terms of lives lost and personal finances drained. The rising cost of health care, housing, and long-term care represent serious challenges that must be solved. But conservatives oppose any tax increases for the wealthy or profitable corporations that might help address these challenges. The GOP’s blind faith in the private sector to solve seniors’ problems has proven woefully misplaced. On the most important issues affecting seniors, Democrats are on seniors’ side.
Unfortunately, seniors have not always voted in their own interests. Voters over 65 went for Donald Trump by four to five points in the 2020 presidential election, despite Trump’s repeated attempts to break his 2016 campaign promise “not to touch” Social Security and Medicare. A poll released in August showed Republicans with a 15-point lead over Democrats among seniors in the upcoming midterms. In fact, seniors as a voting bloc have favored the GOP in every midterm election since 2002.
Political analysts note that seniors have gravitated toward Republicans because of cultural issues, rather than voting in their best economic interests. That’s a raw deal for older voters, says former Fox News commentator Juan Williams: “Republicans did not reward those voters with backing for social safety net programs for seniors – Social Security and Medicare. And they are not backing legislation to cut the cost of prescription drugs.”
With tens of millions of older Americans relying on Social Security, Medicare, Medicaid, and other safety net programs, seniors cannot afford to unconditionally support the party of Ron Johnson, Rick Scott, or Arizona’s Blake Masters. It’s important that older voters know where their candidates truly stand on these vital programs. Seniors should attend town halls with their elected representatives, consume news from credible sources, assess candidates’ actual positions, and cast their ballots wisely. They also can consult our Voters Guide, which rates members of Congress according to their votes on these crucial issues.
Will voters allow the reversal of decades of progress for seniors, the disabled, children and other Americans at risk? Or will we continue to build on the foundation that previous generations put in place to create a more just and equitable society that looks out for its most vulnerable citizens? Seniors, more than any other voting bloc, have the power to answer that question this November—and are among the voters with the most to win or lose.
Max Richtman is president and CEO of the nonprofit National Committee to Preserve Social Security and Medicare. He is former staff director of the U.S. Senate Special Committee on Aging.
NCPSSM Endorses Nevada Democrats as Bulwark Against GOP Attacks on Social Security & Medicare

The National Committee to Preserve Social Security and Medicare officially endorsed all 3 Democratic members of Nevada’s congressional delegation for re-election. During a virtual event on October 20th, NCPSSM President and CEO Max Richtman declared the organization’s support for Representatives Dina Titus, Steven Horsford, and Susie Lee as champions for seniors, with the three members participating live from Nevada.
Nevada is one of the swing states that will determine who controls the next Congress. Richtman said that Reps. Titus, Horsford, and Lee were part of the bulwark against Republican efforts to undermine Social Security and Medicare. All three members of Congress earned a 100% rating on the National Committee’s legislative scorecard.
“Top Republicans have announced their intentions to come after your earned benefits if they regain the majority. They pledged that they would hold the federal government’s debt ceiling hostage unless cuts were made to these programs. The House of Representatives needs fighters who understand that seniors deserve and rely on their earned benefits, and that is why I am so happy to endorse Dina Titus, Susie Lee, and Steven Horsford – and urge that Nevada voters send them back to Congress.” – Max Richtman, NCPSSM President & CEO, 10/20/22
“Max has been telling people for a long time what Republicans are trying to do to Social Security and Medicare,” said Congressman Horsford. “That’s why this election is so important. I don’t want to have to scream it from the mountaintop after the election!”
Rep. Susie Lee vowed to continue the fight for Social Security and Medicare in the 118th Congress. “Republicans want to slash the hard-earned benefits of millions of Nevadans. Not on our watch.”
Richtman said that the three representatives once again proved their commitment to seniors by voting for the Inflation Reduction Act, which will lower prescription drug prices for Medicare beneficiaries – and, hopefully, all Americans.
“Thanks to your representatives’ votes, for the first time in history, Medicare will have the power to negotiate the costs of some of the most expensive drugs, a huge victory for seniors. Their voices also were crucial in securing a cap on the cost of insulin – and on overall out-of-pocket costs for seniors on Medicare Part D.” – Max Richtman, 10/20/22
In accepting NCPSSM’s endorsement, Rep. Dina Titus said, “I can’t tell you how much it means to have the National Committee’s support. This makes it clear who’s fighting for seniors and who isn’t.”

“The House of Representatives needs fighters” for seniors, says NCPSSM President Max Richtman
Political analysts have said that the results of the mid-terms will depend largely on turnout – which party can get out the most voters in key districts across the country. The three Nevada Democrats implored seniors to vote in their best interests, which means casting ballots for the party that will protect – rather than cut and privatize – Social Security and Medicare.
“Control of the House and Senate runs through Nevada. We need every senior in my district to turn out and vote. We are on the front lines of defending our democracy AND the benefits seniors depend on.” – Rep. Steve Horsford, 10/20/22

“I don’t want to have to scream it from the mountaintop after the election.” Rep. Steve Horsford (D-NV) urges seniors to turn out for the mid-terms to protect their earned benefits.
In addition to supporting the three Nevada representatives, the National Committee has endorsed incumbent Democratic Senator Cathleen Cortez Masto, who is in a tight race with former state attorney general Adam Laxalt. Like her three colleagues in the House, Sen. Cortez Masto has a 100% rating on NCPSSM’s legislative scorecard. Laxalt, on the other hand, has said Congress should “find ways… to drive down costs,” which is code for cutting seniors’ benefits.
8.7% Social Security COLA is Highest in Four Decades, But Seniors Need a Better Inflation Formula

The Social Security Administration SSA announced on October 13th that Social Security benefits will increase 8.7 % in 2023 — the largest cost-of-living adjustment (COLA) in four decades. On average, Social Security benefits will increase by more than $140 per month starting in January. Acting SSA Commissioner Kilolo Kijakazi hailed the near-historic COLA:
“Medicare premiums are going down and Social Security benefits are going up in 2023, which will give seniors more peace of mind and breathing room. This year’s substantial Social Security cost-of-living adjustment is the first time in over a decade that Medicare premiums are not rising and shows that we can provide more support to older Americans who count on the benefits they have earned.” – Kilolo Kijakazi, Acting Social Security Commissioner, 10/13/22
Max Richtman, President and CEO of the National Committee to Preserve Social Security and Medicare said in a statement today that the 8.7% COLA is enough to keep seniors from falling further behind, but does not put them ahead financially:
“As helpful as the 8.7% COLA may sound, it’s more like a band aid on a gaping financial wound from chronically rising living expenses for seniors — who have had to make do with historically inadequate COLAs (without a boost in base benefits for the past fifty years). In fact, COLAs have been downright paltry (from zero to 2%) for seven of the last ten years.” – Max Richtman, NCPSSM President & CEO, 10/13/22
NCPSSM’s legislative director, Dan Adcock, told CNBC’s Lorie Konish, “The COLAs really are about people treading water; they’re not increases in benefits… They’re more trying to provide inflation protection so that people can maintain their standard of living.”
A 75 year-old retiree in Florida named Gloria Hinojosa told the New York Times that she relies on her Social Security benefits to cover basic living expenses, including a rent of more than $1,200 per month. She says that the roughly $180 extra she will receive starting in January will give her a little more “breathing room” financially.
The current COLA formula, based on the CPI-W, reflects the impact of inflation on urban wage earners, not seniors. There is a newer inflation index available, the CPI-E (Consumer Price Index for the Elderly), that more accurately reflects seniors’ spending patterns. The CPI-E is included in Rep. John Larson’s Social Security 2100 legislation and in Senator Bernie Sander’s Social Security Expansion Act. Both bills would also give seniors a badly needed benefit boost while requiring the wealthy to contribute their fair share to Social Security. (Republicans have proposed adopting an even less generous COLA formula, based on the Chained CPI, along with cutting benefits by raising the retirement age.)
“Unfortunately, neither bill is likely to come up for a vote during the remainder of the 117th Congress, and that’s a shame. Because every year that Congress kicks the can down the road, the closer Social Security’s projected trust fund shortfall draws — and the more dire the financial struggles become for seniors on fixed incomes. Large majorities of the American public across party lines support Social Security and want to see it expanded and strengthened.” – Max Richtman, 10/13/22
Conservatives claim that the 2023 COLA will add to Social Security’s financial challenges by shortening the life expectancy of the program’s trust fund, an assertion echoed in today’s Washington Post. “The increase will help seniors adjust to higher living costs, but it also will further strain Social Security’s finances, bringing forward the date by which the program’s trust fund is projected to be exhausted.” This, like other pieces of propaganda from the right regarding Social Security, is a red herring. The Chief Actuary of the Social Security program, Stephen Goss, has said that the higher than usual COLA “should have (only) a small effect on trust fund financial status.”
As Max Richtman points out, NCPSSM believes that one of the wealthiest nations in the world can afford to boost benefits for one of its most vulnerable populations.
After years of rising costs for older Americans, a deadly pandemic that took a disproportionate toll on seniors, and rampant post-pandemic inflation, one has to wonder what Congress is waiting for. Seniors and their families should weigh their votes carefully this fall — and elect representatives committed to boosting Social Security – including those frequently inadequate COLAs.”
Congress Gives SSA Enough Funding to Tread Water

Congress passed a continuing resolution Friday to keep the government funded until December 16th. It contains additional money for the beleaguered Social Security Administration, which services the 66 million Americans receiving Social Security and people applying for benefits. NCPSSM president and CEO Max Richtman issued the following statement today in response to the Congressional action:::
“Congress is handing the Social Security Administration a modest financial lifeline, but the extra money may only help the agency to tread water. The Continuing Resolution (CR) to keep the government temporarily funded boosts spending for the Social Security Administration (SSA), an agency that has been chronically under-funded while striving to improve customer service to the public. Under the CR, SSA will receive an additional $400 million for FY 2023. We applaud Congressional Democrats for inserting this funding increase into the bill when spending for most other agencies remains temporarily frozen.
The increased funding should help SSA cope with its long-standing customer service backlog, which was greatly exacerbated by the pandemic. Customers have been subjected to long hold times on the SSA toll-free phone line, extensive delays awaiting disability claims hearings, and – since the re-opening of field offices last summer – waiting in line at some locations for hours in the heat. With the new level of funding, those problems likely will not get worse, but they may not significantly improve.
SSA requested twice as much funding for the CR ($800 million) and Congress shouldapprove that level when an Omnibus Appropriations bill for the reminder of FY 2023 is enacted. We will work with Social Security champions in Congress and other advocacy groups to secure SSA the funding it truly needs to improve customer service. American workers whose wages finance the Social Security program expect Congress to fully fund SSA so it can properly serve the public.” – Max Richtman, President and CEO, National Committee to Preserve Social Security and Medicare, 9/30/22
Last May, the House Ways and Means Social Security subcommittee held a hearing on customer service issues at SSA. Witness after witness (including NCPSSM President Max Richtman) testified that the agency is in dire need of additional resources in order to properly serve the public. While witnesses praised SSA employees for doing their best to provide the public with customer service during the pandemic, they painted a picture of an underfunded and overworked agency in desperate need of Congressional action.
Rebecca Vallas of the Century Foundation advocacy group told lawmakers at the hearing, “A decade-plus history of congress underfunding SSA’s already incredibly lean operating budget, worsened by the pandemic, has spurred several urgent crises in the agency’s customer service…The casualties are your constituents.”
Among the most pressing problems that have plagued SSA customer service are long hold times, disconnects, and busy signals on the agency’s toll-free phone line and excessive delays in Social Security Disability Insurance (SSDI) hearings. (Over 100,000 claimants have died waiting for their cases to be adjudicated.). In April, SSA was able to re-open most of its field offices after being shuttered for almost two years during the COVID pandemic.
“We are doing what we can with current staff and funding. The demand for service is high; we are losing staff; and morale is low,” testified Peggy Murphy, Director of the Social Security field office in Great Falls, Montana. “SSA is at a critical juncture as we face the future.”
In August, Lorie Konish of CNBC reported:
People who face long waits for service at the Social Security Administration’s field offices have had to contend with one more complication this summer — intense heat. “Although most SSA field offices can assist visitors, in some locations people have been standing outside in the heat for hours at a time, without the guarantee of getting their needs met,” wrote Reps. Richard Neal, D-Mass., and Kevin Brady, R-Texas, in a letter addressed to Kilolo Kijakazi, acting commissioner of the Social Security Administration. – CNBC, 8/17/22
“To avoid waiting in line, I strongly encourage people who can to use our online services at www.socialsecurity.gov, call us and schedule appointments in advance rather than walking in without an appointment,” said SSA Commissioner Kilolo Kijakazi in a statement. “Phone appointments can save you a trip to a busy office.” SSA also outlined several steps it was taking to reduce wait times at field offices.